Raimonds Liepins: “Maybe this will be the biggest match ever but for sure it will be an ARM WRESTLING WAR.”
Source: Voice of Armwrestling

Raimonds Liepins: “Maybe this will be the biggest match ever but for sure it will be an ARM WRESTLING WAR.”
Source: Voice of Armwrestling

Check out this interesting video from Voice of Armwrestling about Alan Zoloev!
Source: Voice of Armwrestling

Tendon Healing
How is Tendinopathy Treated?
In most cases, you can start treating a tendon injury at home. To get the best results, start these steps right away:
Tendon healing can be largely divided into 3 overlapping phases, inflammatory repairing and remodelling phases:
The initial inflammatory phase, which lasts about 24 hours, erythrocytes, platelets and inflammatory cells (eg: neutrophils, monocytes and macrophages) migrate to the wound site and clean the site of necrotic materials by phagocytosis. In the meantime, these cells release phaso active and chemo tactic factors which recruit tendon fibroblast to begin collegan synthesis and deposition.
A few days after the injury, the repairing phase begins. In this phase, which lasts a few weeks, tendon fibroblast synthesise abundant collegan and other extra cellular matrix components such as proteoglycans and deposit them at the wound site.
After about 6 weeks, the remodelling phase starts. This phase is characterised by decreased cellularity and decreased collagen and glycosaminoglycan synthesis. During this period, the repair tissue changes to fibrous tissue, this again changes to scar like tendon tissue after 10 weeks. During the later remodelling phase covalent bonding between the collagen fibres increases resulting in repaired tissue with highest stiffness and tense our strength. Also, both the metabolism of tenocytes and tendon vascularity decline.
During tissue healing growth factors play an important role in this process.
1: Platelet Derived Growth Factor (PDGF) is produced shortly after tendon injury and stimulates the production of other growth factors.
2: TGF-beta is active during the inflammatory and repair phases of tendon healing. TGF-beta plays a major role in the repair of injured tendons. TGF-beta 1 aids an extra cellular matrix deposition; however, it’s over expression results in tissue fibrosis. TGF-beta 2 functions similarly to TGF-beta 1. However, TGF-beta 3 has been shown to improve tissue scarring. Peak levels of TGF-beta receptory expression occur at day 14 post injury and decrease until day 56 post injury.
It should be noted that, except for degenerative tendons (tendonosis), injured tendons tend to heal. However, the healing tendon does not reach the biomechanical properties of the tendon prior to surgery.

Subscribe to channel for more armwrestling videos
This is most common place where injuries happen and most common mistake while armwrestling. Tips from pros on how to not get your arm broken in armwrestling.
Down is compilation video on arm breaks in armwrestling. All these arm breaks could have been avoided. Knowing armwrestling technique would decrease your chances of getting injured or your arm broken.
Some things that are common in all theses arm break videos:
– Pushing not Pulling
– Facing away from arm
– Moving Shoulder in front of arm
https://www.youtube.com/watch?v=VRYQf2TNm-w

Name: Raimonds Liepiņš ➫
|
||
Nickname: Coach |
||
Birthdate: 22 February 1990 |
||
Country: Latvia 🇱🇻 |
||
| — XSportNews.com — Measurements — XSportNews.com — | ||
Height: 169 cm (5’6.5″) |
||
Weight: 75.6 kg (167 lb) |
||
Biceps 💪 |
Forearm |
Wrist |
40 cm (15.75″) |
36 cm (14.2″) |
20 cm (7.9″) |
| — XSportNews.com — — XSportNews.com — | ||
Preferred armwrestling technique(s): LEFT arm – Triceps press, RIGHT arm – Hook/Side press
Preferred hand: Left arm
When and how did you start armwrestling: When I started high school (2006) met some guys who competed in armwrestling competitions. I loved to have challenge so I went to couple competitions and every time placed in medals with my left arm. When I finnished High school (2010) armwrestling was already part of my life. Big influence for me being in armwrestling were Rūdolfs Cīrulis and Jānis Amoliņš. Started working as armwrestling coach in 2012. 2013 – Vice president of Latvian Armwrestling Federation, 2014 started my club “Legacy”, Coach of Latvian national team since 2014. 2015 – President of Latvian Armwrestling Federation, Latvian armwrestling trainer of year 2017.
Armwrestling record (best results):
Armwrestling projects: Armwrestling projects in Latvia and Armwrestling Training by Ray – Youtube channel
My success are my students/atheletes:
Kaspars Grāvis – multiple medalist EuroArm and World Championship
Sandra Zālīte multiple medalist EuroArm and World Championship
Vladislavs Krasovsakis 3x Junior World Champion (in 2017 5 silver medals and 1 gold from EuroArm And WCH 2018)
More than 50 national champions
Armwrestling goal: Goal has always been to win. But since I started training others my goal has been to help others win. My biggest succes is being able to help others achieve their dreams.
Toughest match: Every year at least one. Can’t pick favorite, but you can watch below a video with my latest toughest match vs. DZMITRY MIKHEI.
Toughest opponent(s): Injuries.
Occupation: Personal trainer for strength sports, Gym owner, President of Latvian Armwrestling Federation.
What motivates you: Great feeling that comes from helping others achieve their dream or just help them.
Preferred armwrestler(s), someone who you really admire in armwrestling: Jānis Amoliņš – true legend. And I`m not just talking about what he does on table but more about how much hard work is put in his success.
Favorite quote / an idea that guides you in life: Luck is the last dying wish of those who want to believe that winning can happen by accident. Sweat on the other hand is for the ones who know it`s a choice. So decide now, because destiny waits for no man. So when the time comes and a thousand different voices are trying to tell you: you are not ready for it, listen instead to that lone voice of descent, one that says you are ready, you are prepared, it’s all up to you know.
Where do you see yourself in 10 years from now: Right here. Not going anywhere.
Message to your fellow armwrestlers / pullers: If you want to achieve something you have to work for it. If nature hasn`t given you best genetics hard work will make you earn them. Nothing is impossible you just have to find best path for You.
RAIMONDS LIEPINS VS JANIS AMOLINS – LATVIAN NATIONALS 2016
Raimonds Liepins – RIGA OPEN 2017 LEFT OPEN 3rd place
RAIMONDS LIEPINS VS DZMITRY MIKHEI – WORLD CHAMPIONSHIP 2017
________
INFO: This is 5th armwrestler profile made on XSportNews. Many more profiles of armwrestlers / pullers will follow this one. If you have very good results in armwrestling or you are promoting armwrestling in different projects, you can send your profile to XSportNews – Facebook page.
Tendinopathy (tendon injuries) can develop in any tendon of the body.
Typically, tendon injuries occur in three areas:
Non-insertional tendinopathies tends to be caused by a cumulative microtrauma from repetitive overloading eg overtraining.
Tendons are the tough fibres that connect muscle to bone. Most tendon injuries occur near joints, such as the shoulder, elbow, knee, and ankle. A tendon injury may seem to happen suddenly, but usually, it is the result of repetitive tendon overloading. Health professionals may use different terms to describe a tendon injury. You may hear:

Tendinitis (or Tendonitis): This actually means “inflammation of the tendon,” but inflammation is actually normal tendon healing response which can cause some tendon pain. This is known as the reactive phase and is a good tendon healing response.
The problem really occurs when you healing rate is less than your injury rate – known as tendon dysrepair – which is when tendinopathies can quickly deteriorate into the degenerative (cell death) phase. This is characterized by collagen degeneration in the tendon due to repetitive overloading. These tendinopathies therefore do not respond well to anti-inflammatory treatments and are best treated with functional rehabilitation. The best results occur with early diagnosis and intervention.
What Causes a Tendon Injury?
Most tendon injuries are the result of gradual wear and tear to the tendon from overuse or ageing. Anyone can have a tendon injury, but people who make the same motions over and over in their jobs, sports, or daily activities are more likely to damage a tendon.
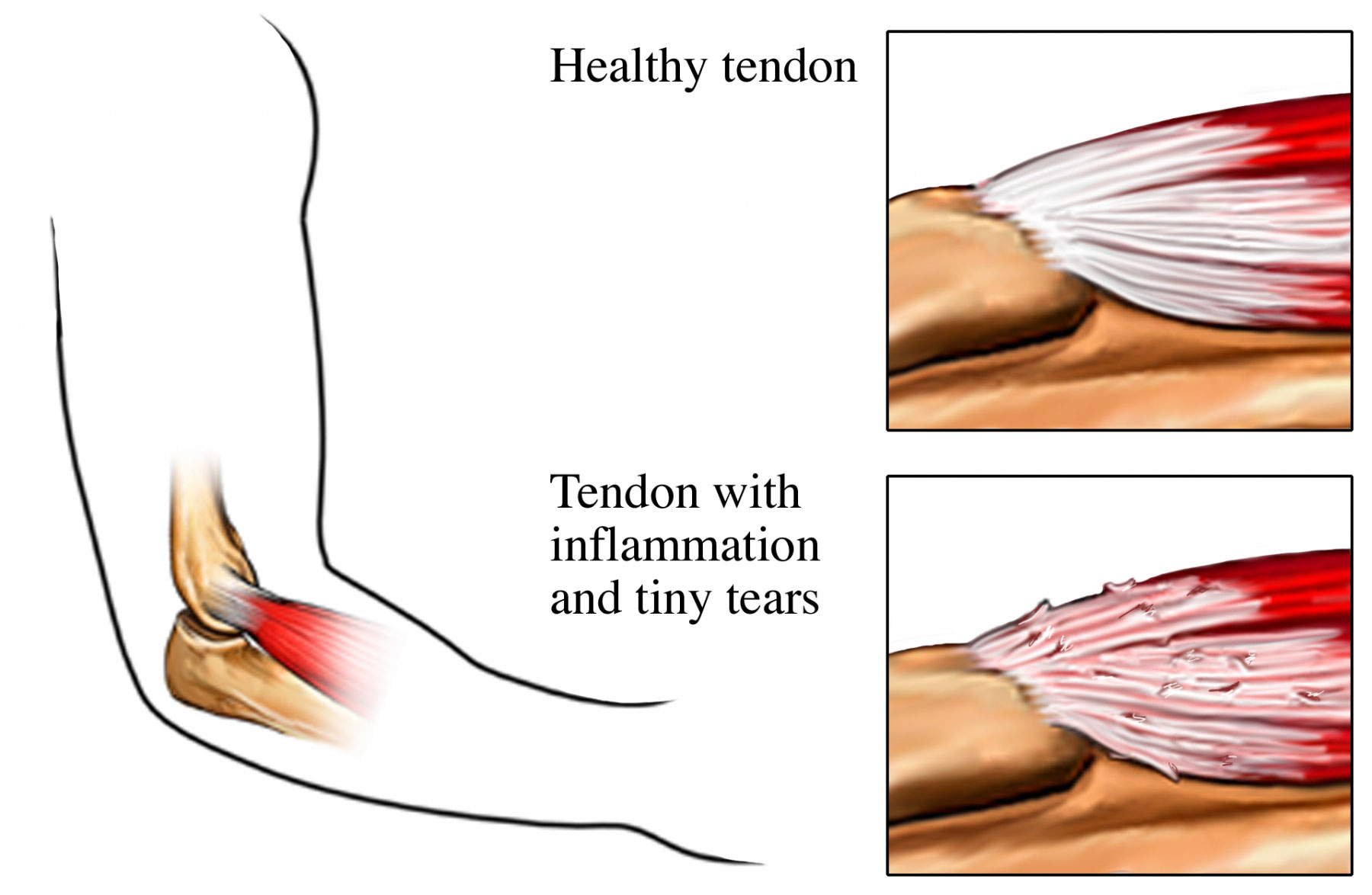
Your tendons are designed to withstand high, repetitive loading, however, on occasions, when the load being applied to the tendon is too great for the tendon to withstand, the tendon begins to become stressed.
When tendons become stressed, they sustain small micro tears, which encourage inflammatory chemicals and swelling, which can quickly heal if managed appropriately.
However, if the load is continually applied to the tendon, these lesions occurring in the tendon can exceed the rate of repair. The damage will progressively become worse, causing pain and dysfunction. The result is a tendinopathy or tendinosis.
Researchers current opinion implicates the cumulative microtrauma associated with high tensile and compressive forces generated during sport or an activity causes a tendinopathy.
For example, in explosive jumping movements, forces delivered to the patellar tendon can be eight times your body weight. Cumulative micro trauma appears to exceed the tendon’s capacity to heal and remodel.
Tendinopathy usually causes pain, stiffness, and loss of strength in the affected area.
The symptoms of a tendon injury can be a lot like those caused by bursitis.

The inability of your tendon to adapt to the load quickly enough causes tendon to progress through four phases of tendon injury. While it is healthy for normal tissue adaptation during phase one, further progression can lead to tendon cell death and subsequent tendon rupture.
It is very important to have your tendinopathy professionally assessed to identify it’s injury phase. Identifying your tendinopathy phase is also vital to direct your most effective treatment, since certain modalities or exercises should only be applied or undertaken in specific tendon healing phases.
To diagnose a tendon injury, your physiotherapist will ask questions about your past health, your symptoms and exercise regime. They’ll then do a physical examination to confirm the diagnosis. If your symptoms are severe or you do not improve with early treatment, specific diagnostic tests may be requested, such as an ultrasound scan or MRI.
For more Armwrestling videos click this button:

These muscles are largely involved with pronation. The superficial muscles have their origin on the common flexor tendon. The ulnar nerve and artery are also contained within this compartment.The flexor digitorum superficialis lies in between the other four muscles of the superficial group and the three muscles of the deep group. This is why it is also classified as the intermediate group.
Pain in different place of your arm can be caused by a lot of factors. But if pain is located on your muscle there is a big chance it`s a tight spot or trigger point. Armwrestling involves a lot of same movements from gripping (wrist and finger flexion). Any kind of moment that has been overdone can cause muscles to get tight. In this video we are showing some ideas about how to do self massage on your forearm flexor muscles using specific equipment and using things you can find in almost any gym. If your forearms get tight try these and leave a comment did it help.
For more Armwrestling videos click this button:
The muscles of the forearm can be divided into two groups: anterior (flexors) and posterior (extensors).Both the flexors and extensors are further divided into superficial and deep layers.The forearm muscles that control the movement of the hands are known as extrinsic hand muscles. These muscles originate outside the hand and insert on structures within it.
Shown here, the extrinsic hand muscles are the flexor carpi radialis, palmaris longis, flexor carpi ulnaris, and flexor digitorum superficialis.These muscles move the wrist, hand, fingers and thumb.The pronator teres inserts on the radius and pronates the forearm and hand.
The superficial muscles in the anterior compartment are the flexor carpi ulnaris, palmaris longus, flexor carpi radialis and pronator teres. They all originate from a common tendon, which arises from the medial epicondyle of the humerus.
Flexor Carpi Ulnaris
Palmaris Longus
This muscle is absent in about 15% of the population.
Dissection Tip: Just distal to the wrist, if you reflect back the palmaris longus, you will find the median nerve immediately underneath it
Flexor Carpi Radialis
Pronator Teres
The lateral border of the pronator teres forms the medial border of the cubital fossa, an anatomical triangle located over the elbow.
The flexor digitorum superficialis is the only muscle of the intermediate compartment. It can sometimes be classed as a superficial muscle, but in most cadavers it lies between the deep and superficial muscle layers.
The muscle is a good anatomical landmark in the forearm – the median nerve and ulnar artery pass between its two heads, and then travel posteriorly.
There are three muscles in the deep anterior forearm; flexor digitorum profundus, flexor pollicis longus, and pronator quadratus.
Flexor Digitorum Profundus
Flexor Pollicis Longus
This muscle lies laterally to the FDP.
Pronator Quadratus
A square shaped muscle, found deep to the tendons of the FDP and FPL.

Myofascial release (MFR, self-myofascial release) is an alternative medicine therapy that claims to treat skeletal muscle immobility and pain by relaxing contracted muscles, improving blood and lymphatic circulation, and stimulating the stretch reflex in muscles.
Fascia is a thin, tough, elastic type of connective tissue that wraps most structures within the human body, including muscle. Fascia supports and protects these structures. Osteopathic theory proposes that this soft tissue can become restricted due to psychogenic disease, overuse, trauma, infectious agents, or inactivity, often resulting in pain, muscle tension, and corresponding diminished blood flow.
Myofascial release focuses on reducing pain by easing the tension and tightness in the trigger points. It’s not always easy to understand what trigger point is responsible for the pain. Localizing pain to a specific trigger point is very difficult. For that reason, myofascial release is often used over a broad area of muscle and tissue rather than at single points.
All things I`m using in video you can find by clicking on picture.
FOAM ROLLER

Nano Triggerpoint Roller

Myofascial Release Ball

For more Armwrestling videos click this button:
https://youtu.be/JtfHw8NyEGw
Raimonds Liepiņš – Coach RayX
INSTAGRAM: https://www.instagram.com/coach_rayx/
FACEBOOK: https://www.facebook.com/coach.rayx
TWITTER: https://twitter.com/RaimondsLiepins
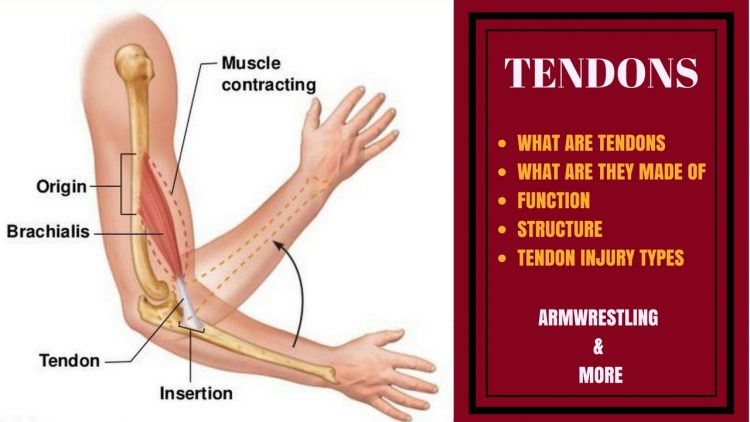

Tendons
Tendons are situated between bone and muscles and are bright white in colour, their fibro-elastic composition gives them the strength require to transmit large mechanical forces. Each muscle has two tendons, one proximally and one distally.

Tendons are connective tissue, group of tissues in the body that maintain the form of the body and its organs and provide cohesion and internal support. The connective tissues include several types of fibrous tissue that vary only in their density and cellularity, as well as the more specialized and recognizable variants—bone, ligaments, tendons, cartilage, and adipose(fat) tissue.

The dry weight of each wall of tendons is made up of more than 95% of collagen. The ends of tendons, which are the most solid parts, are composed almost exclusively of collagen, up to 99%. Our tendons’ properties and functions are directly related to the architecture and quality of the collagen fibres. The collagen portion is made up of 97–98% type I collagen, with small amounts of other types of collagen
The structures surrounding the tendon can be split into 5 subcategories. The main aim of these structures is to reduce friction and enable the tendon to glide smoothly. This is an important factor for ensuring the transitions of the force is at its most efficient.

Tendon functions
The tendons’ main role is to transmit forces from the muscle to the bone and absorbs external forces to prevent injury to the muscle. As the tendon runs from a very compliant tissue (the muscle) to a ridged stiff one (the bone), this role can become very difficult, this can result in strain concentrated at the site of merging tissues. This can be a common site of injury.
The make up of the tendon is now not thought to be the same throughout, research has discovered that the tendon itself may be more ridged in some parts and more compliant and elastic in others to overcome this concentration of strain and risk of injury. Each tendon will differ throughout the body depending on the rate in which they are strained. The behaviour of the collagen within the tendon depends on the intramolecular types, quantity and bond.

Tendon injuries
Collagen contributes to keep the structure and strength of tendons. When collagen breaks down, small tears appear in the tendon, weakening it and causing pain. Tendinitis notably affects those who perform repetitive tasks in their jobs, sports or daily activities. Another example of a disease related to tendons is bursitis. Bursitis is the swelling of the bursa, a small fluid-filled sac that allows muscles to glide easily over other muscles as well as bones. When you hurt a joint or tendon or use it excessively, the bursa may swell, causing pain, redness and a burning sensation.
For more Armwrestling videos click this button:

Pain in elbow from armwrestling movements is nothing new. We all have experienced different kind of pain in elbow joint sometimes it`s tendons but sometimes its one or many of muscles involved in movement. With this video we are starting series that focus on things that could cause pain in elbow. Today we are talking about muscle named Pronator Teres. it`s main function is to pronate arm and flex elbow. Sometimes from all pronation and elbow flexion this muscle can get tight and shorten what you need to do is to release it with trigger point active release techniques. you need to release it. It can cause pain in medial epicondylus and in muscles surrounding your elbow, also numbness in fingers. All symptomes can cause something called Pronator Teres Syndrome.

Pronator teres syndrome is a compression neuropathy of the median nerve at the elbow. It is rare compared to compression at the wrist (carpal tunnel syndrome) or isolated injury of the anterior interosseous branch of the median nerve (anterior interosseous syndrome).
The most common cause is entrapment of the median nerve between the two heads of the pronator teres muscle. Other causes are compression of the nerve from the fibrous arch of the flexor superficialis, or the thickening of the bicipital aponeurosis.
The median nerve passes through the cubital fossa and passes between the two heads of pronator teres muscle into the forearm. It then runs between flexor digitorum superficialis and flexor digitorum profundus muscles and enters the hand through the carpal tunnel.

The pronator teres has two heads—humeral and ulnar.
The median nerve enters the forearm between the two heads of the muscle, and is separated from the ulnar artery by the ulnar head.
The muscle passes obliquely across the forearm, and ends in a flat tendon, which is inserted into a rough impression at the middle of the lateral surface of the body of the radius, just distal to the insertion of the supinator.
The lateral border of the muscle forms the medial boundary of the triangular hollow known as the cubital fossa, which is situated anterior to the elbow.
Take a look at the following picture of two men arm wrestling, paying close attention to the position of the forearm of the person who is winning this match.
The name of the pronator teres gives away its function. Pronation refers the inward rotation of a body part towards the middle of the body. Since the pronator teres is located in the forearm, its function is to rotate (pronate) the forearm inward. Think back to the arm wrestling example from the beginning of the lesson; an arm wrestler must internally rotate (pronate) their forearm in order to pin the arm of their opponent.
The pronator teres is not only used during arm wrestling; this muscle is used hundreds of times each day. Performing simple tasks like brushing your teeth, combing your hair, and eating all require forearm pronation, and therefore require the use of the pronator teres. The pronator teres also functions to flex the forearm, which involves bending the arm at the elbow joint.
For more Armwrestling videos click this button:

Have you experienced pain in middle of your upper arm after armwrestling in a brachialis muscle. From all the rotation and tension that is put on this muscle sometimes it will tighten up and won`t let go. Stretching this muscle is almost impossible but you can try (for stretching scroll down). If stretching won`t work try release techniques used in video (scroll down). We use these techniques to get rid of pain in upper arm or brachialis muscle. We recommend you to invest in foam roller or physio ball (tennis ball will do it). Injuries can put you back by weeks or even years and your armwrestling career will suffer. This muscle is important to Load-up and Toproll or basically all armwrestling movements. Keep your arms healthy and your Toproll and Hook pain free.
The brachialis (brachialis anticus)
The brachialis is a long and strong muscle of the upper arm. It originates at the distal half of the anterior side of the humerus. In addition, the origin tendon attaches to the medial and lateral intermuscular septa of the arm, two dividing membranes separating the flexor from the extensor muscles. Distally the muscle inserts at the tuberosity of the ulna where its’ fibers are also connected to the joint capsule.
Brachialis Function
The primary function of the brachialis muscle is to flex the forearm. Flexion of the forearm is the same motion used to perform bicep curls, which involves bringing the hand upward by bending at the elbow. Contrary to what you might think, the brachialis is actually stronger than the biceps brachii and functions as the primary flexor of the forearm.
You perform forearm flexion constantly each day. For example, you must flex your forearm in order to armwrestle, eat, drink, brush your teeth, and bathe (imagine trying to perform all these daily tasks without bending your elbows). Because the brachialis muscle is used so frequently, it oftentimes becomes irritated, inflamed, or damage from overuse.

VIDEO with Release techniques.
For more Armwrestling videos click this button:
Some of You will need to do this only one time but some will have to work on it. When you do any of these release techniques don`t do any armwrestling or exercises that cause pain. Doing more exercises or armwrestling will stop healing processes. Once pain is gone go back to armwrestling.
Try stretching together with release techniques
Standing Stretch

Step 1
Stand in a doorway with your shoulders parallel to the doorway’s opening.
Step 2
Reach straight to the side and slightly back to grasp the doorjamb at shoulder level with your right hand. Back further away from the doorjamb, if necessary, so you can fully straighten your right arm.
Step 3
Turn your body slowly toward the left until you feel a stretch in your upper right arm. Hold the stretch for 15 to 30 seconds, breathing normally, then switch to the other side. Do the stretch a total of three to five times on each side.
Seated Stretch

Step 1
Sit down on the floor. Straighten both arms, and plant your hands on the floor behind you, slightly wider than your hips. Turn your hands so your fingers point straight back.
Step 2
Scoot your hips slowly forward, keeping your weight evenly distributed, until you feel mild tension in your biceps and brachialis. You might feel a stretch across your chest, too.
Step 3
Hold the stretch for 15 to 30 seconds, breathing normally, then scoot your hips back toward your hands to release the stretch. Repeat a total of three to five times.
Raimonds Liepiņš - Coach RayX